 – First10EM")
Preparation for intubation, appropriate preoxygenation, and preventing peri-intubation arrests has been one of my core topics for conference talks. My initial airway series emphasized “optimizing the basics” and carefully considering “is this patient ready for intubation?”. My “RSI and then they die” lecture is by far my most watched video on YouTube. Following the advice and expertise of Scott Weingart, I have been a big fan of using BiPAP during the preoxygenation phase, but the evidence base for that practice has always been rather weak. (To be fair, I am not sure you need a lot of evidence to see the difference between starting an intubation with the sats at 100% as compared to 88%. However, aspiration and other complications are risks to consider with prolonged noninvasive ventilation.) Thankfully, published today (I was given early access), we have the Pragmatic Trial Examining Oxygenation Prior to Intubation (PREOXI trial), the first large RCT looking at noninvasive ventilation for preoxygenation, and I think it might be a practice changer for many people.
The paper
The PREOXI trial: Gibbs et al. Noninvasive Ventilation for Preoxygenation during Emergency Intubation. NEJM. (Will update the official citation when I have it, but at the time of writing and scheduling this blog post, the paper is not officially published.) NCT05267652
The Methods
The PREOXI trial was a multicenter, unblinded randomized trial from 7 emergency departments and 17 ICUs in the United States.
Patients
Critically ill adult patients undergoing intubation with sedation and a laryngoscope were eligible.
Exclusions include prisoners, pregnant patients, patients already on noninvasive ventilation, apnea or hypopnea, need for immediate intubation precluding randomization, and if the clinician performing the procedure thought that NIPPV was either needed or contraindicated.
Intervention
Preoxygenation with noninvasive positive pressure ventilation (NIPPV).
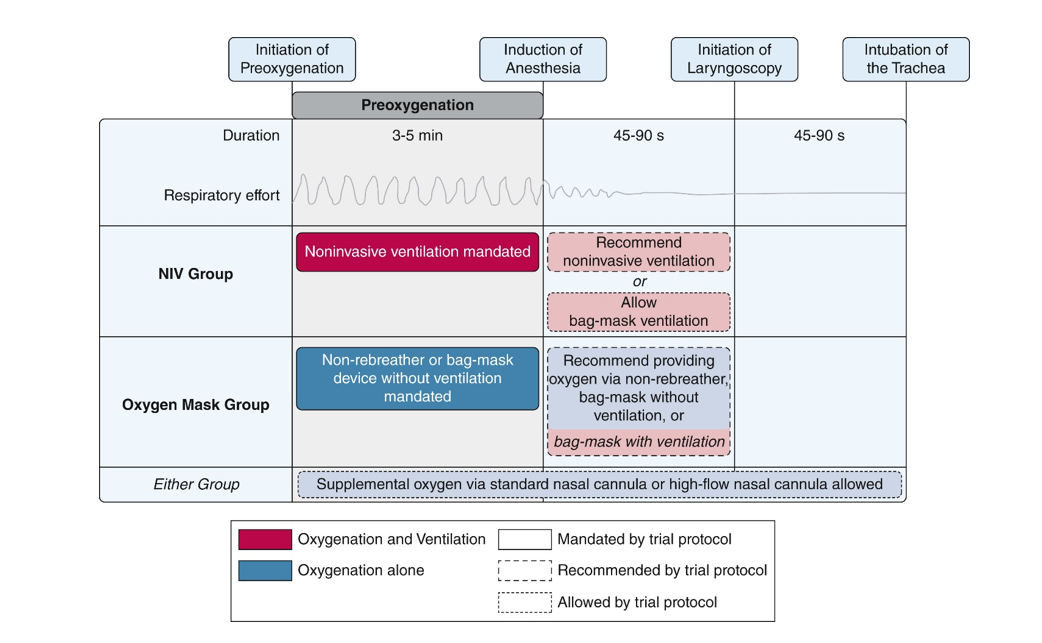
“The trial protocol provided best-practice recommendations for preoxygenation with noninvasive ventilation, including instructing operators to (1) administer noninvasive ventilation from the start of preoxygenation until the initiation of laryngoscopy, (2) set an FiO2 of 100%, (3) set an expiratory pressure of at least 5 cm H2O, (4) set an inspiratory pressure of at least 10 cm H2O, and (6) set a respiratory rate of at least 10 breaths per minute.”
Comparison
Preoxygenation with oxygen mask. (The choice between nonrebreather and BVM was left to the clinician.)
“The trial protocol provided best-practice recommendations for preoxygenation with an oxygen mask, including instructing operators to (1) administer supplemental oxygen through the oxygen mask from the start of preoxygenation until the initiation of laryngoscopy and (2) administer the highest flow rate of oxygen available (≥ 15 L/min).”
Shared procedures
Both groups were instructed to preoxygenate for at least 3 minutes (if feasible). Both groups were allowed to use a BVM after induction of anesthesia. Both groups were also allowed to use additional nasal prongs or high flow nasal oxygen throughout the procedure.
Outcome
The primary outcome was peri-intubation hypoxemia, defined as an oxygen saturation of less than 85% during the interval between induction of anesthesia and 2 minutes after intubation.
The Results
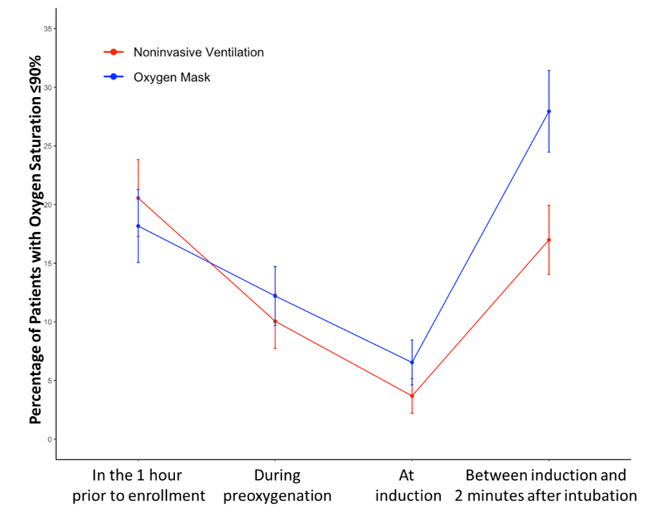
They assessed 4567 patients and enrolled 1301. The mean age was 61, and about half of patients were presenting with hypoxemic respiratory failure. 86% of intubations were performed by a resident or fellow, with clinicians having a median of 50 prior intubations. Most patients were treated in line with their group assignment (96% on the NIPPV group and 99% of the mask group). 8% of the NIPPV group and 17% of the mask group had an oxygen saturation of less than 95% at the time of induction of anesthesia (which is likely not a baseline imbalance, but rather a marker than NIPPV provides better preoxygenation.)
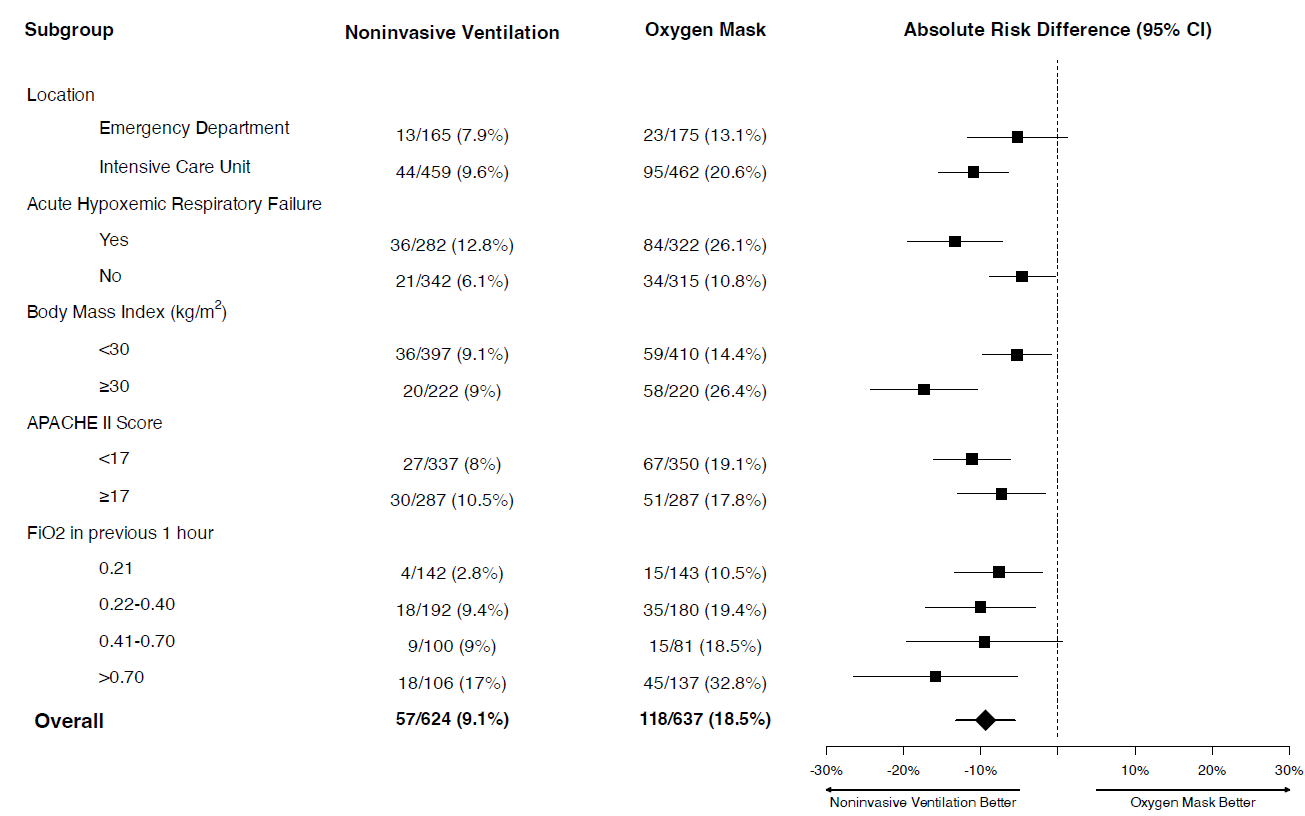
For the primary outcome, NIPPV resulted in significantly less peri-intubation hypoxemia (19% vs 9%, ARR 9.4%, 95% CI 5.6 to 14.2, p
An oxygen saturation of less than 70% occurred in 15 patients (2.4%) in the noninvasive ventilation group and in 36 patients (5.7%) in the oxygen mask group (absolute risk difference, -3.2 percentage points; 95% CI, -5.4 to -1.1).
Cardiac arrest between induction of anesthesia and 2 minutes after tracheal intubation occurred in 1 patient (0.2%) in the noninvasive ventilation group and 7 patients (1.1%) in the oxygen mask group (absolute risk difference, -0.9 percentage points; 95% confidence interval, -1.8 to -0.1). (Stopping the clock at 2 minutes might be a little early to see the true impacts on an intervention on cardiac arrest. Furthermore, the simple transition to positive pressure ventilation can result in hemodynamic collapse in some patients, and so I think they should have started recording cardiac arrest from the moment that preoxygenation started.)
There was no difference in aspiration rates (0.9% with NIPPV and 1.4% with mask).


My thoughts
We have become accustomed to large high quality trials from this airway group (which includes Brian Driver), but it truly is a massive accomplishment to run a study of this size in critically ill patients. This trial asks an important question, and I think gives us a practice changing answer, although if you watch my RSI and then they die talk, it will be clear that I already sort of believed this, and therefore I am probably very biased to accept results that coincide with my beliefs.
As far as pretest probability goes, these results make sense. NIPPV should improve oxygenation as compared to face mask oxygen. At baseline, this trial was much more likely to be successful than trials of novel chemicals, such as paxlovid, and therefore we should be somewhat more willing to change practice based on these results, despite some obvious limitations.
The trial was not blinded. The oxygen saturations were recorded by a research assistant, and not the clinical team, and oxygen saturations are relatively objective. However, we all know that saturations are not perfectly objective, and in the setting of a poor waveform, we all have the capacity to reject numbers that we don’t believe. Although it would have added a layer of complexity, it would not have been impossible to blind this nonclinical observer, and that would have made the trial a lot stronger.
I think the primary outcome they used here is a good outcome, and an outcome that I care about. It is, of course, a surrogate monitor based outcome, but a surrogate outcome with strong associations with real clinical outcomes. (And the most important clinical outcome, peri-intubation arrest, was also improved, although that was just an exploratory secondary outcome.) However, a slight mental adjustment needs to be made, because the absolute benefit in this trial refers to brief hypoxemia, and only a fraction of those patients will have real clinical harm. For my practice, that adjustment doesn’t matter much. However, in resource limited settings, that adjustment will probably be key when performing a cost benefit analyses. For all of us, that adjustment will probably be the key variable that influences your opinion on whether NIPPV should become standard care or be used selectively after this trial.
Although it is very common, especially in pragmatic trials, I always have a problem with clinicians being allowed to exclude patients because they think the intervention is either needed or contraindicated. You are allowing clinicians to presume the results of the trial, which biases the results. In this trial, they had already excluded all the patients who were on NIPPV at the time of enrollment, which really should have encapsulated all of the patients where the clinician thought that NIPPV was needed. Therefore, this part of the exclusion was probably unnecessary. However, this subjective exclusion has the potential to exclude the exact patients who need NIPPV, biasing the results towards the null hypothesis, while also excluding the patients who are at highest risk of adverse events, biasing the results away from demonstrating harm. Those are the two questions we really need answered, and the exclusion criteria used limit our ability to answer both.
248 patients were excluded because of agitation that ‘precluded NIPPV’, but with the technique of delayed sequence intubation, we know that agitation is not really a contraindication to NIPPV.
A short note on publication bias. I have never before been given early access to a paper. In fact, I have never been sent a paper by any author, at any state of publication. I was honoured to be considered (which I supposed could bias my review). However, my bigger concern is all the other trials that would never be sent. Is the author of a negative trial going to work hard to get the results into my hands for a review? Seems unlikely. In this way, the medical community spends a lot more time talking about positive research than negative, which is a form of publication bias, even if both papers are ultimately published.
Again, I think this trial is probably practice changing. There is a clear benefit, and despite the possible sources of bias, the pretest probability is strong enough to believe these results. There is no indication of harm. However, one should always be cautious changing practice after a single unblinded trial. Furthermore, there are issues of cost to consider, and most of my patients don’t need NIPPV in the preoxygenation phase. Much like delayed sequence intubation, I think the real question is not whether we should be doing this, but rather when this technique is required? I am not sure this needs to be used routinely, for all patients. Many of my patients are clearly fine with just flush rate oxygen by nonrebreather, and implementing this for all intubations would increase cost and resource utilization dramatically without necessarily providing a corresponding benefit. My take, unrelated to this data, and unchanged from previous, is that if my patient has any indication of shunt, primarily identified by patients who have an oxygen saturation less than 96% despite being on flush rate oxygen by nonrebreather, I will use NIPPV to preoxygenate. However, if the patient has an oxygen saturation of 100% on a nonrebreather, I don’t think NIPPV is necessary.
Bottom line
This unblinded, multicenter RCT demonstrates less peri-intubation hypoxia (as well as potentially less peri-intubation cardiac arrest) when using NIPPV for preoxygenation, and I think the results are practice changing, although exactly who needs this technique remains an open question.

{kind=link}

Other FOAMed

Emergency Airway Management Part 1: Optimizing the basics
Emergency Airway Management Part 2: Is the patient ready for intubation?
Evidence based medicine is easy
Evidence based medicine resources