
(UroToday.com) The 2024 American Society of Clinical Oncology (ASCO) annual meeting featured a session on prostate cancer, and a presentation by Dr. Anthony Joshua discussing results of the MAST study, a randomized, double-blind, placebo-controlled trial of metformin for reducing progression among men on expectant management for low-risk prostate cancer. Active surveillance involves vigilant monitoring of selected prostate cancer patients, with radical treatment initiation upon significant disease progression. Active surveillance eligibility varies, generally including low-risk prostate cancer men. Metformin is a biguanide anti-hyperglycemic agent that was FDA approved in 1994 and is known for its excellent efficacy in diabetes management. Generally, metformin is well tolerated, but 30% of patients do have gastrointestinal adverse effects, can lead to B12 deficiency, and rarely is associated with lactic acidosis. There is extensive rationale for utilization of metformin in this patient population from a biological, epidemiological, and clinical standpoint:
The goal of this study is to examine the effect of metformin on the rates of progression among men with low-risk localized prostate cancer on active surveillance.
MAST was a randomized double blind placebo controlled trial carried out in 12 centers across Canada. Eligible patients had biopsy-proven, low-risk, localized prostate cancer diagnosed within the past 6 months, with a Gleason score of 1/3 of total cores involved, at least 50% of any one core involved, or Gleason pattern 4 or higher). The trial design for the MAST trial is as follows:

From a statistical standpoint, the assumption was 45% disease progression at 36 months, powered to detect a HR 0.63. The power calculation was 80% power, at a 2 sided type error of 0.05, adjusted for 6% loss to follow-up. The sample size of 408 (204 patients per group) was chosen for 145 progression events. Finally, progression free survival was assessed by the Kaplan Meier method and the log rank test to assess differences by exposure. Multivariable Cox proportional hazards analysis was used for assessing predictors of progression. Key exclusion criteria were: (i) previous prostate cancer treatment, (ii) current and/or previous use of the 5-alpha reductase inhibitors (within the past 6 months), (iii) current and/or previous use of metformin, sulfonylureas, thiazolidinediones, or insulin, (iv) diagnosis of type 1 or 2 diabetes, and (v) any condition with an increased risk of metformin-associated lactic acidosis.
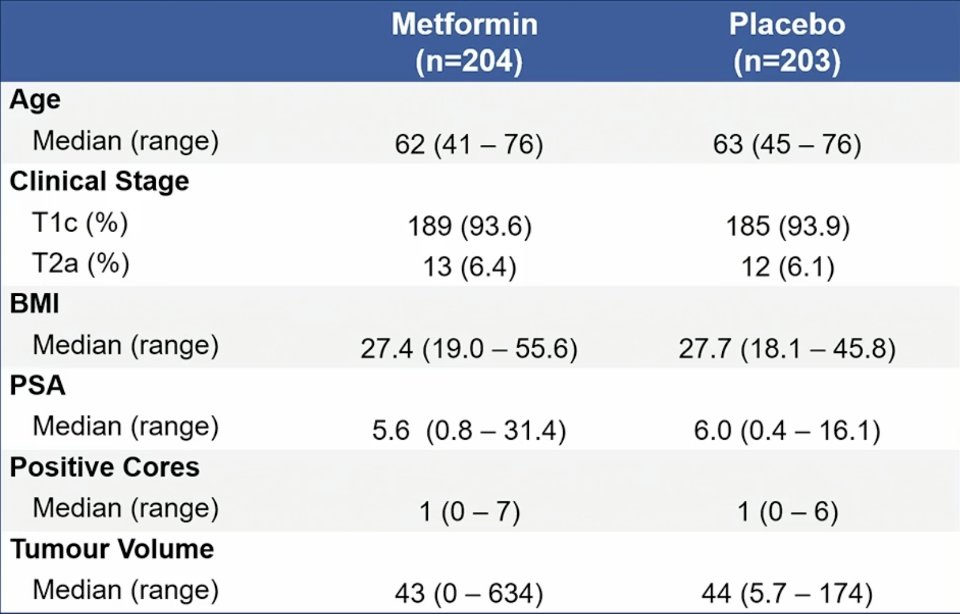
Between October 2013 and December 2023, 407 patients were enrolled in MAST, of which 204 were administered metformin and 203 received a placebo. Baseline demographics were well balanced between the two groups, highlighted as follows:
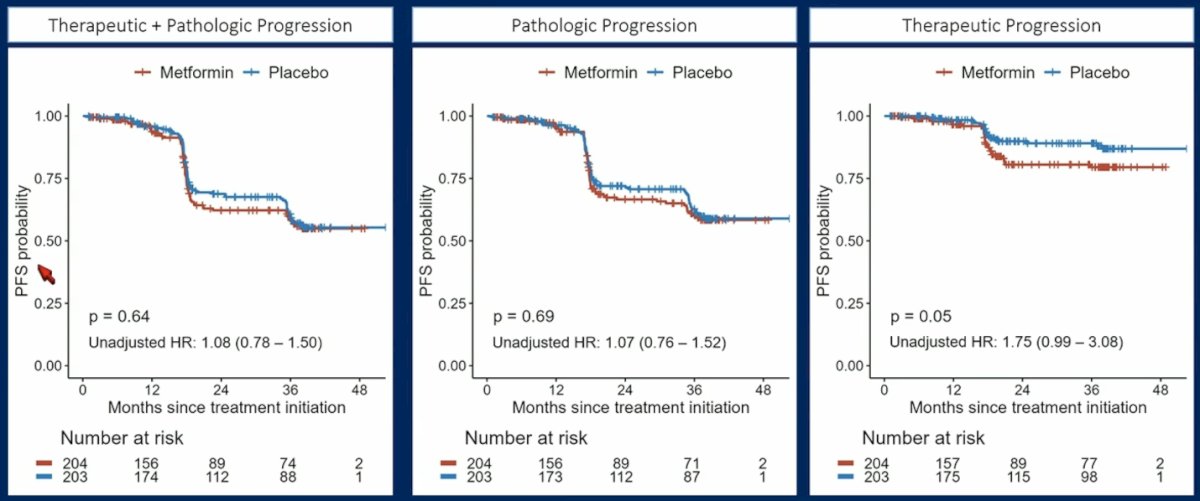
Overall, 141 patients experienced disease progression. There was no statistically significant difference in progression-free survival observed between patients treated with metformin and those receiving placebo with regards to therapeutic + pathologic progression (HR 1.08, 95% CI 0.78-1.50), pathologic progression (HR 1.07, 95% CI 0.76-1.52), or therapeutic progression (HR 1.75, 95% CI 0.99-3.08):
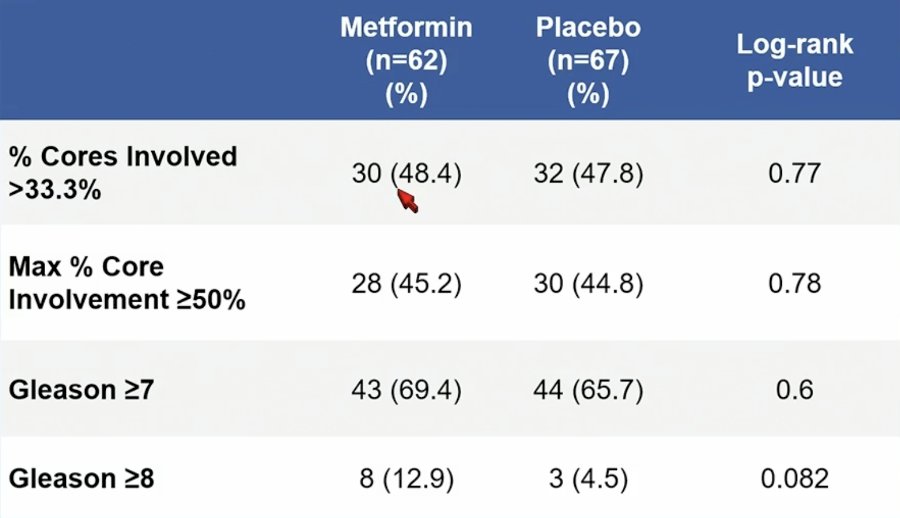
Taking a closer look at pathologic progression endpoints, there was no statistically significant differences, although Gleason >= 8 disease was more common in the metformin (12.9%) versus the placebo (4.5%) group (p = 0.082):
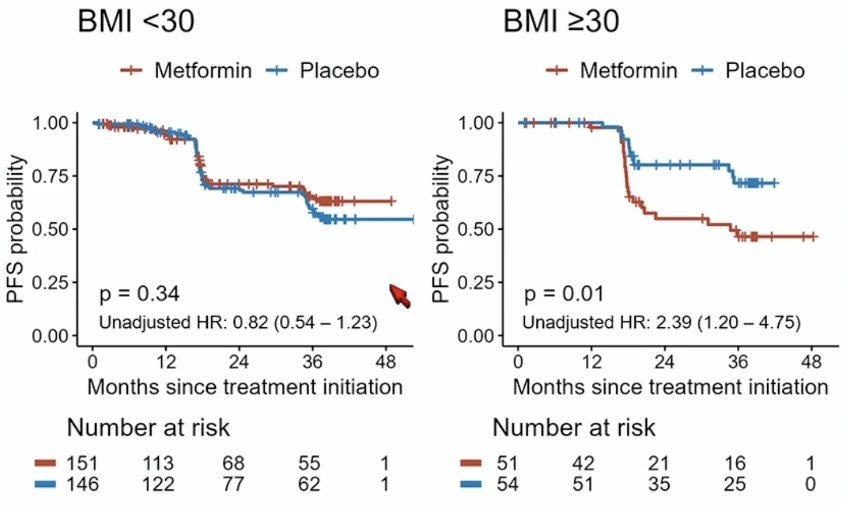
Interestingly, patients with a BMI >= 30 had a worse progression free survival probability (HR 2.39, 95% CI 1.20-4.75; interaction p = 0.01) with metformin:
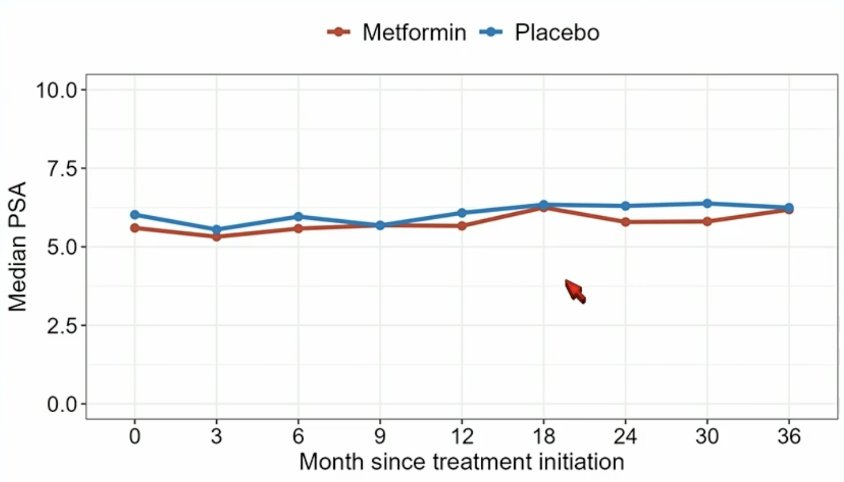
On multivariable analysis, baseline PSA (HR 1.08, 95% CI 1.02-1.14), number of positive cores (HR 1.46, 95% CI 1.19-1.80), and log prostate volume (HR 0.68, 95% CI 0.53-0.88) were predictors of pathologic progression. PSA kinetics were similar between the metformin and placebo groups:
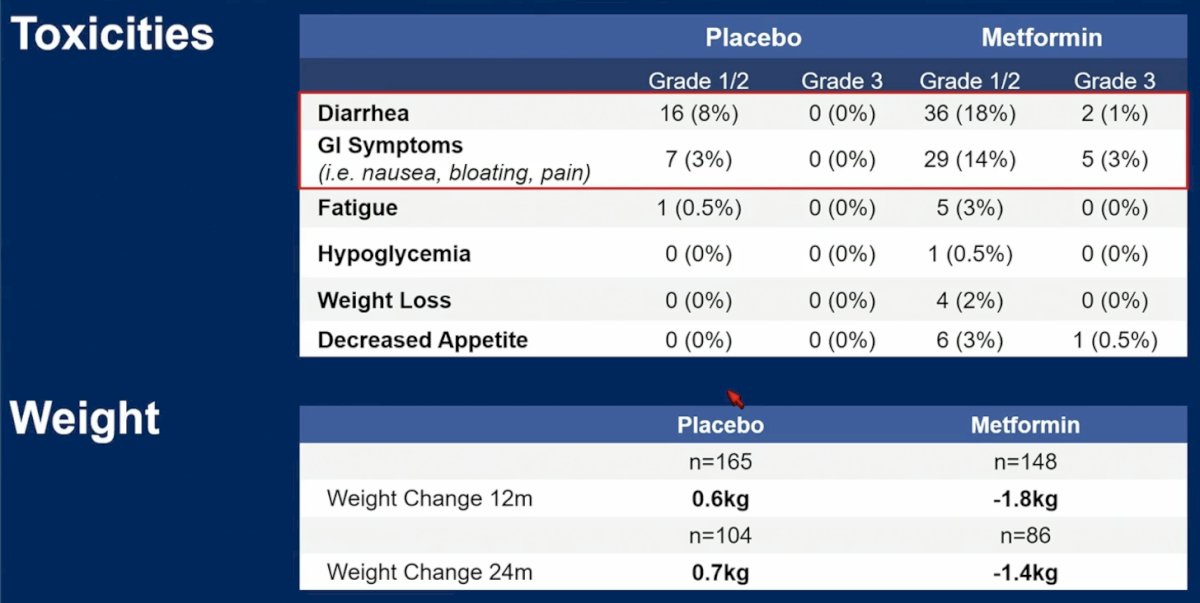
Toxicity data for each group, as well as changes in weight over the course of the trial are as follows:
Dr. Joshua noted several limitations of the MAST trial:
- A 10 year accrual window
- MRI use changed routine practice since study initiation
- MRI use was not controlled for during the study
- There were recruitment challenges during the study (ie. COVID interruptions)
- There was limited ethnic diversity (7%)
Future research from the MAST study will including (i) clinical subgroup analyses to see if outcomes are aligned with serum biomarkers and tissue genomics, (ii) patient reported outcome analyses to determine bio-psycho-social factors that contribute to active surveillance adherence and therapeutic progression including anxiety and regret, (iii) proteomic and metabolomics analyses to assess the relationship with metabolic signaling and metformin targets, and (iv) artificial intelligence analyses to develop an algorithm for predicting progression.
Dr. Joshua concluded his presentation discussing results of the MAST trial with the following take home messages:
- Metformin use does not prevent progression of low-risk localized prostate cancer suitable for active surveillance
- Exploratory subgroup analyses indicate potential detriment to patients with high BMI at study entry, and patients with Grade 4+ at progression
- Further research is needed to understand the consequences of metformin on prostate cancer outcomes
Presented by: Anthony M. Joshua, MBBS (Hons), PhD, BSc (Med) (Hons), FRACP, St. Vincent’s Hospital Sydney, Sydney, Australia
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2024 American Society of Clinical Oncology (ASCO) Annual Meeting, Chicago, IL, May 31st – June 4th, 2024